
Cognitive analytic therapy (CAT): how might it help me?
Escrito por:
Cognitive analytic therapy (CAT) is a time-limited therapy, which is usually offered in courses from 16 to 24 weekly sessions.
CAT looks at the problematic ways in which a patient thinks, feels and acts, and at the events and relationships from the patient’s past (particularly from childhood), which may shape their thoughts and behaviours in the present and stop them leading fulfilling lives.
We spoke to one of our top psychologists, Dr Nicky Kimber-Rogal, all about CAT therapy and how the treatment works.

What is cognitive analytic therapy (CAT)?
CAT is a time-limited, focussed therapy developed at Guy’s Hospital, London, in the 1980s by Dr Anthony Ryle. At a time when long-term therapy or analysis was very expensive, this therapy offered patients the opportunity to increase well-being through NHS resources and in a shorter time span.
Ryle based this therapy on patients he saw in his GP practice whose presenting symptoms were often psychological rather than physical. He introduced the idea of reciprocal roles (aspects of the individual learned in childhood from their primary caretakers, and the child’s reactions to these). He noted three types of unproductive patterns of thinking, feeling and acting, which kept patients stuck.
He called these traps (circular ways of doing things that always ended up with the same result); dilemmas (‘black and white’, ‘either/or’ thinking); and snags (self-limiting, defeatist ways of coping).
- Traps involve repetitive and self-confirming negative self-identity strategies.
- Dilemmas involve viewing only polarised choices as options.
- Snags involve self-defeating procedures.
How does CAT differ to cognitive behavioural therapy (CBT)?
The main difference between CAT and CBT is that CAT includes attachment patterns learned in childhood (see below).
Reciprocal roles
Reciprocal roles are made up of cognitive (thinking), affective (feeling) and behavioural (acting) aspects. During therapy, so-called ‘faulty beliefs’ - extreme statements such as “I must be universally liked by others to be accepted” - are explored and challenged.
Internal parent (IP) and internal child (IC) roles are collections of thoughts, feelings and actions; the first group are said to be the internalised active behaviours and characteristics of adults around us and the second, our reaction to these adults.
CAT is a “no-blame” therapy in that it does not criticise any adult or carer; rather, it shows how non-adaptive coping strategies can be learned, for example, from an influential sibling, school teacher or another authority figure.
Coping strategies work at the time in childhood but are often redundant, cause and maintain problems in adulthood. Therapy also takes into account that, even if the person has had a traumatic environment, there may have been a significant figure or figures in their life with whom they formed a close and safe bond and therefore protected them.
Development of roles
Step 1
The first type of learned role play is self-to-other, based on the original parent-to-child interaction, and is interpersonal; for example, a “critical parent” to a child who then feels “not good enough” (see fig.1).
Step 2
The child internalises both parent and child roles and plays them out within the self. This sets up a self-to-self interaction and is intrapersonal. For example, the child can become very self-critical, and consequently cannot tolerate further criticism from others (see fig. 2).
Step 3
The third part of the process is when the child also learns that they can act out the parent (IP) role, independent of the child (IC) role, towards others. This is another self-to-other or interpersonal interaction where the individual can feel, for example, critical or contemptuous towards others: “I don’t suffer fools gladly” (see fig.3).
Figure 1: Active internal parent role to receptive internal child role
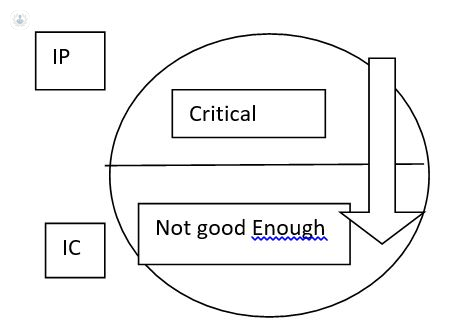
Figure 2: The child internalises both roles which are then played out intrapersonally.
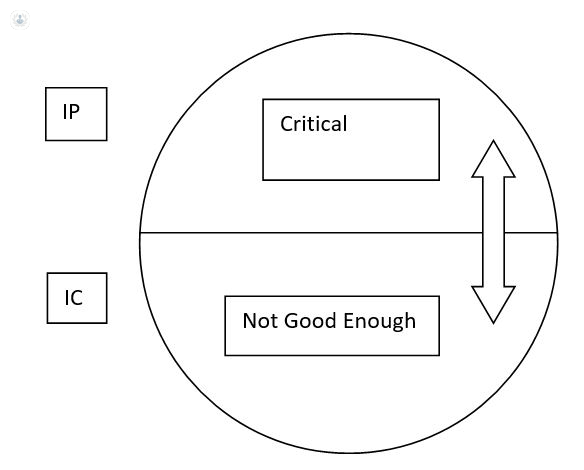
Figure 3: The child learns to play out both roles in relation to others (again, an inter-personal procedure) - usually with someone who consciously or unconsciously knows one or other, similar roles.

To summarise…
In summary, the feeling, thinking and behavioural repertoire of the person have become very limited. Firstly, because there are only limited roles learned; secondly, because the roles can become acted out in an extreme way: we become used, for example, to only playing the very critical or very `not good enough’; or very passive/bullied or very angry/bullying. There is no room for spontaneity and creativity.
CAT and attachment theory
CAT emphasises attachment processes. From the moment we are born we are all “in relation” to another, and these early interactions can set the tone for later life. That does not mean they cannot be altered or adjusted, it just means that sometimes, when things are not going well for us as adults, we need to look at where and how the problems started.
Attachment theory (see Bowlby) is also a part of CAT and is basically a ‘spatial’ theory: “when I am closed to my loved one, I feel safe”. Bowlby identified two basic types of early attachment: secure and insecure.
If the carer is present and generally able to provide for the child, they tend to grow up secure and confident – ready to explore the world, their feelings and their capabilities.
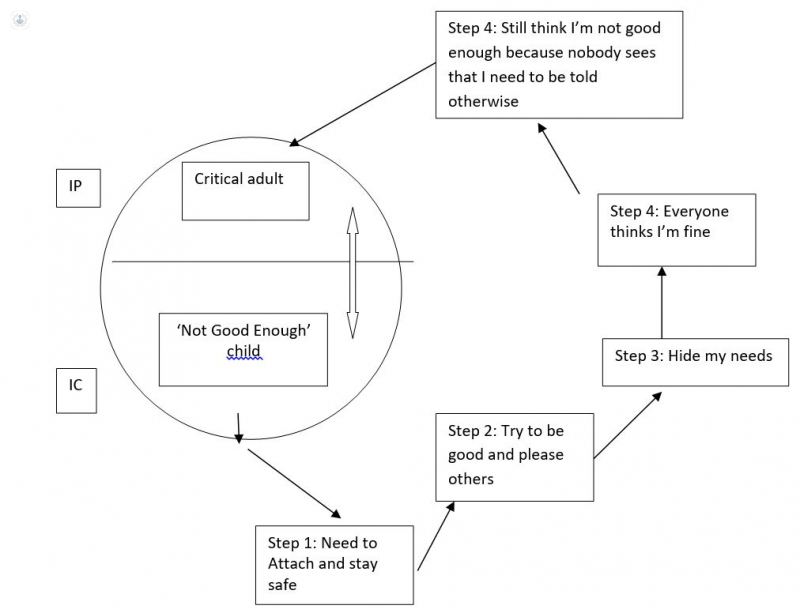
If the child is insecure, they may resort to, for example, people-pleasing and perfectionism and ignore their own needs. Because these needs are ignored and become hidden, they tend not to ask for things nor express themselves, other people think they’re fine and don’t offer to help or understand them. It becomes a vicious cycle.
How does therapy ‘work’?
Clients come to therapy because they are distressed in some way. Usually, the therapist will write down the presenting problem (PP) and the target problem (TP) – for example, a presenting symptom may be anxiety or lack of confidence, and the target problem could be anything from “I don’t know how to make a presentation at work” or an inability to work through an unhappy relationship. Often, the client will be asked to bring a narrative to the second session (a brief account of their lives, and significant people and events in it).
CAT is helpful for many people in that it uses diagrams to focus on what the basic difficulties may be (see below). Patterns can then be tracked in everyday situations – becoming aware of habits is the first step.
CAT uses ‘the 3 R’s’: recognition, reformulation (understanding how patterns have developed) and revision (changing patterns that were once useful in childhood but not productive later on).
Figure. The beginnings of a typical CAT diagram
What are the benefits of CAT?
CAT is very collaborative in that the therapist and client work together on possible alternative strategies and the therapist earnestly and openly explores patients’ subjective meanings. Open discussion is the key, and there is no ‘client-patient’ hierarchy. The client can be asked at various points in therapy, is it:
- Useful
- Meaningful
- Helpful
- Hopeful.
People can often get into the habit of presenting only their ‘performance self’ rather than one that they feel is ‘weak’ but is, in fact, entirely human and understandable: we all have strengths and weaknesses and need to learn from each in one way or another.
They can find themselves trapped in an outer performance self, which can be created when they try to deny the existence of natural tendencies, such as anger, assertiveness, joy, hostility, jealousy, aggression, drive, interest. But that doesn’t mean that these feelings vanish – they may just become projected on to somebody else.
Although patterns such as people-pleasing were ‘adaptive’ at the time (e.g. playing the good child or the smooth, unruffled schoolboy), the strategies can wear out in the longer term and people get taken advantage of and remain unrecognised.
They are only adaptive in the sense that they produced a quasi-sense of attachment through, for example, placatory behaviour or self-denigration. This allowed the individual to allay the biggest and most powerful drive: fear and loss of the one on whom they were once, as children, dependent for life.
However, it is short-term gain only: in the longer term, they find they have entered the second stage of wretchedness: a state of alienation, divorced from the core self and therefore living `outside their life’: `sold out’ in attempts to live in a procedural persona.
This second place is a very unpleasant place to be, where the dawning of being a ‘divided self’ emerges and where the solution (via the procedures/coping strategies) has become the problem. However, once recognition and understanding have been explored, the revision of redundant strategies can become an exciting exploration of the future.
ii. A statement to which Ellis (see Rational Emotive Therapy) attributes much of human suffering.
If you would like to know if CAT is the right therapy in your case, you can book an appointment with Dr Kimber-Rogal now via her Top Doctor’s profile here.

