
What is Dupuytren’s disease?
Escrito por:Dupuytren’s disease or Dupuytren’s contracture is sometimes called the ‘Viking disease’ because it is most commonly found in countries which were invaded by the Vikings. It is a common disease affecting the hands, which usually presents itself in middle age or later in life and is more common in men than women. Mr James Nicholl walks us through this condition and how it can be treated.

Underneath the skin of the palm of the hand and extending into each finger is a sheet of fibrous tissue, called fascia. This tissue acts as a shield to protect the delicate structures underneath from the minor trauma of everyday life. The fascia also anchors itself to the overlying skin, so that the skin of the palm doesn’t slip when you grip things.
In some people, groups of cells in the fascia sheet develop small lumps. These lumps can develop into cords, the fibres within them contract and pull the fingers down towards the palm. It mostly affects the ring fingers and little fingers.
Who gets Dupuytren’s disease?
The largest group with this disease are those with a family history of the condition. However, it is also thought to be associated with liver malfunction, anti-epileptic medication when taken over a long period of time, and is more common in diabetics.
Many patients, however, have none of these risk factors. Often the condition begins later in life and progresses slowly. The more aggressive form of the disease affects people at a much younger age and advances rapidly.
Can Dupuytren’s disease be prevented or delayed?
There is nothing you can do to delay the advance of the disease, but how quickly it progresses is very variable. Medical intervention is only necessary once hand function becomes impaired. When a person can no longer place their hand flat on a table top, we usually recommend treatment.
When all four fingers have severe Dupuytren’s contracture, treatment for this is difficult and is less likely to result in a good outcome.
Treating Dupuytren’s contracture
Treatment is only recommended when a contracture has developed such that the palm cannot be placed flat on a surface and the fingers cannot be straightened beyond 30 degrees of flexion. There are a variety of treatment options available. One treatment involves an injection of an enzyme (Xiapex) into the hand tissue, followed by a manipulation a day or two later. The hand is bandaged after the injection and the patient advised not to use it. Swelling, bruising and soreness are to be expected.
After 24-48 hours, the patient will return to the hospital to have the palm injected with a local anaesthetic and the finger/fingers gently manipulated to be straight. The hand will be bandaged again for 24 hours and the patient will be encouraged to move the fingers and use the hand as much as possible. The initial bruising and soreness will settle after a few days. The patient will be referred to a hand therapist to exercise the hand and a splint will be worn at night for up to three months. This treatment is most effective when the Dupuytren’s is confined to the palm.

flexion contracture of the metacarpophalangeal
joint of the ring finger.
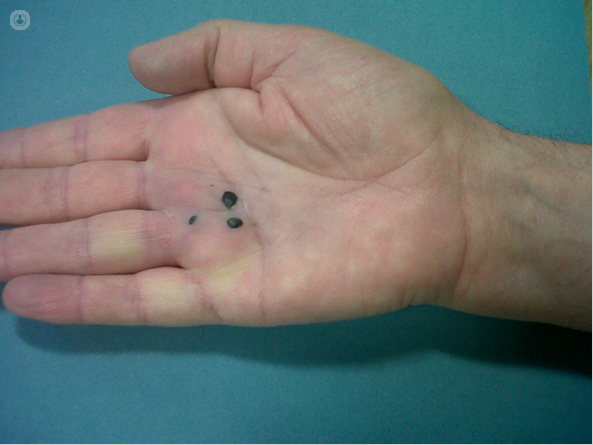
The finger now straightens fully.
The black spots are blood blisters which will rapidly resolve.
Another method of treatment is dividing the cord with a needle that is inserted through the skin called a needle fasciotomy. For more advanced disease and when the cord extends into the finger, surgery is usually recommended. The surgery is called a palmar fasciectomy which involves the removal of the diseased fascia or tissue. The skin is separated from the underlying lumps and cords of the tissue, isolating and protecting the nerves and arteries that supply the fingertips and then the affected tissue is removed.
Surgery is usually carried out as a day case procedure, under general anaesthetic or a regional block where the patient is awake but the arm is completely numb. A zigzag incision is made from the palm into the finger, and the cord of Dupuytren’s excised.
Post-surgery, patients are fitted with a plaster of Paris beneath heavy bandages to hold the fingers straight. After a few days, the patient has postoperative physiotherapy with a hand therapist. The bandages are removed, and a splint made which must be worn at night for up to three months to stop the fingers from flexing towards the palm. The stitches will be removed two weeks after the operation.
20% of patients will experience temporary numbness following the surgery, but there is only a 1 in 100 chance that this numbness will be permanent. Some patients may experience stiffness, swelling and pain. Dupuytren’s disease can recur and there is a small risk of infection.
Mr James Nicholl is an orthopaedic surgeon in Tunbridge Wells. Visit his Top Doctors profile for more information or to book an appointment.


