
TAMIS – a new approach in colorectal surgery
Autore:Transanal minimally-invasive surgery (TAMIS) is a cutting-edge technique used to remove larger, more complex rectal polyps or early stages of rectal cancer. Ms Sarah Mills, a leading colorectal surgeon, explains how this procedure works, its success rate and the aftercare required following surgery.
What is transanal minimally-invasive surgery (TAMIS)?
TAMIS is what we call natural orifice surgery. This means that we perform the surgery through a natural opening on the body, which in this case, is the anal canal. By inserting a small port and effectively doing keyhole surgery through it TAMIS is an organ-sparing surgery in that it avoids the need to remove larger sections of the bowel containing a polyp or an early cancer. Therefore, there is less impact on bowel function and in some cases, it can avoid the need for a permanent stoma.
How does the procedure work?
If you are thought to be a suitable candidate for TAMIS, you will be asked to come to hospital to have the procedure which is performed under a general anaesthetic. When we do the operation, we put a small port into the anal canal and we attach a gas supply to inflate the rectum so that we have a nice view of the lesion we need to remove. We then use some long laparoscopic instruments, including a cutting device, a retractor, and some scissors to remove the lesion in its entirety. We then extract it through the port. We normally check again to make sure there is no bleeding and put some local anaesthetic into the area to keep you more comfortable afterwards. Most people only need to spend one night in hospital after this procedure and find it to be really quite comfortable.
Who would make a good candidate for TAMIS?
There are two main groups of people who would make a good candidate for TAMIS. Firstly, older people who have lots of medical problems who would be very high risk for having a long general anaesthetic and a major operation to remove their early cancer or even their polyp. The second group is anyone else who has an early rectal cancer or a large complex rectal polyp who does not want to have a larger operation, or someone with a very low lesion, who wanted to avoid the necessity of having a permanent stoma.
If you have been diagnosed with a rectal cancer or polyp and want to know if you are suitable for this procedure, your scans, endoscopy and biopsy results will need to be assessed in a specialist multidisciplinary team (MDT). Here, we sit down with a surgeon, a radiologist, an endoscopist, an oncologist and often a pathologist to make an assessment of all the information about your lesion and to see whether you will be suitable for this. Sometimes it is necessary to repeat a scan or an endoscopy as we look for specific things to see if the lesion could be removed by this technique. Not all rectal cancers or polyps are suitable for this and this is based on a specialist assessment.
What’s the success rate of the procedure?
It is difficult to put hard figures on the success rate of the procedure because this is relatively new, so there is not a lot of published literature about it. However, most people feel that it is successful at moving large polyps and even early cancers without an unacceptably high risk of recurrence or leaving residual disease behind.
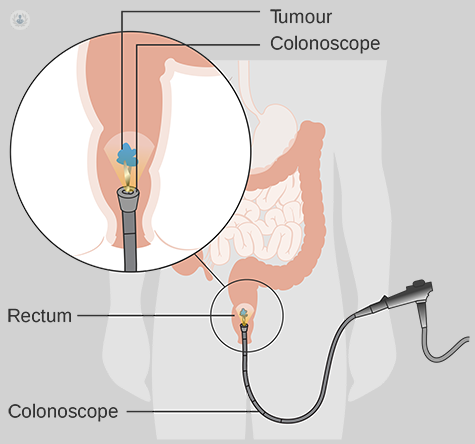
One of the main advantages of it is that, unlike removing lesions like this with a colonoscope which removes the lesion in several pieces, the TAMIS technique removes the lesion on block, in one piece, so that we can be sure if there is a cancer within it, it has been completely removed. In addition to this, because this technique involves removing only a small portion of the wall of the bowel as opposed to a long segment of the bowel with major surgery, it has a lot less impact on bowel function (i.e. how your bowel works afterwards).
What happens after surgery?
After the surgery, you will be asked to stay in hospital overnight so we can properly monitor you and make sure you are comfortable before you are discharged. After you have gone home, the specimen that has been removed will be sent to the pathologist to be examined under the microscope. It usually takes about a week or so to get the results back from this. What happens next depends on whether the specimen was a benign polyp or if there was a cancer within it.
Everybody will have a further endoscopic test to check the site where the lesion was removed has completely healed three months further down the line from the operation. If your polyp was completely benign, the only further surveillance you will need is regular future colonoscopies to make sure you have not grown any more. If there was a cancer in the lesion removed, you may require further treatment. This might be surgery or possibly chemotherapy or radiotherapy. The nice thing about TAMIS is that it does not preclude any of those further treatments. You will then be put into a five-year cancer surveillance programme that involves having CT scans, colonoscopies and tumour marker blood tests at regular intervals to be sure that the cancer has not recurred.
To find out more about rectal cancer and polyp removal, make an appointment with an expert.

