
Trigeminal neuralgia – how ‘the worst pain known to man’ can be managed
Autore:Trigeminal neuralgia is a chronic pain condition that affects the trigeminal nerve, which is located on the face. The incidence of trigeminal neuralgia generally increases with age, but it is an uncommon condition with 4.3 people affected per 100,000 per year, on average. Incidence is slightly higher in women. Trigeminal neuralgia is described as being brief, short-lasting episodes of pain that are electrical or stabbing in nature in one or more divisions of the trigeminal nerve on the face. This is an extremely debilitating condition and it is one that Dr Jim Blackburn, a pain medicine specialist, is an expert in diagnosing and treating.

What causes trigeminal neuralgia?
The main causes of trigeminal neuralgia are:
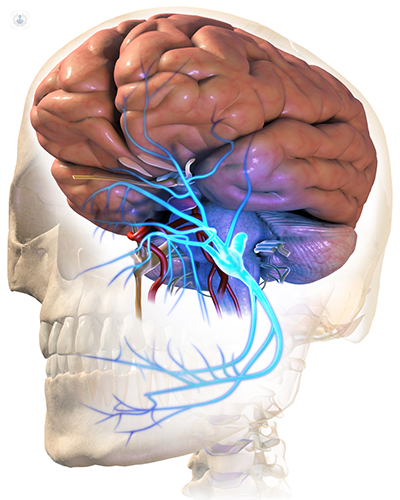
- Neurovascular conflicts – this is when blood vessels in the brain put pressure on the trigeminal nerve. For example, pulsations of blood vessels can put pressure on the trigeminal nerve, triggering an episode of pain.
- Secondary causes – trigeminal neuralgia can also be associated with people suffering from multiple sclerosis (MS) and brain tumours, however, the latter is much rarer.
What can trigger trigeminal neuralgia?
Further to the underlying causes of trigeminal neuralgia, actual episodes of pain can be triggered by:
- Talking
- Touching the face
- Brushing your teeth
- Hot or cold drinks
- Chewing
- Cold wind on the face
- Flexing at the hips (e.g. when tying your shoelaces)
Due to the everyday triggers of trigeminal neuralgia, they are extremely difficult and impractical to avoid. This is why treatment is necessary to manage and relieve pain episodes.
People often confuse other forms of facial pain with trigeminal neuralgia, but what defines this condition is that the pain comes in brief bursts, which can be described as an electric shock. If you are experiencing facial pain that cannot be described in such a way, it is unlikely to be attributable to trigeminal neuralgia. A specialist would be able to determine this with a thorough physical examination and assessment of your medical history.
What can be done for managing pain caused by trigeminal neuralgia?
Trigeminal neuralgia has several treatment options, each with their own benefits and associated risks. The following are the most viable treatments available:
- Medication – anti-epileptic drugs, such as carbamazepine can be prescribed to calm down the misfiring of the trigeminal nerve. As the pain caused by trigeminal neuralgia is nerve-related, traditional painkillers will not work to manage this. Whilst medication can work to relieve pain, this can be short-lived, and hence medication is usually a first step toward having surgery or injection treatments.
- Injections to the gasserian ganglion – this is known as gasserian gangliolysis and involves the injection of either glycerol, heat or a balloon into a collection of nerve cells called the gasserian ganglion. This lies inside the skull on both sides of the head and from here the trigeminal nerve separates into three different branches. This is performed with general anaesthesia.
- Surgery – e.g. microvascular decompression surgically removes or repositions blood vessels responsible for compressing the trigeminal nerve which can relieve pain episodes. Radiosurgery using a gamma knife can be used to focus radiation at the root of the trigeminal nerve which reduces or eliminates pain.
When you are diagnosed with trigeminal neuralgia, you will have a brain scan with contrast to show the instances of blood vessel and nerve conflicts (i.e. where pain stems from on the trigeminal nerve), as well as signs of multiple sclerosis or brain tumours. Treatment can then be guided by a combination of these scan results and the patient’s comorbidities. For example, a patient that has other health problems is unlikely to be suitable for surgery and patients whose trigeminal neuralgia is caused by their MS are not likely to benefit from surgery either.
The main treatment that I offer to my patients is gasserian gangliolysis which aims to stop pain in 90-95% of patients in the first round of treatment. In the few cases where this treatment is not successful, additional treatment sessions can be given. When it is successful, the effects of pain relief can last between 1-5 years.
Can Botox be used to treat trigeminal neuralgia?
There are some studies that indicate the use of Botox in treating trigeminal neuralgia and relieving pain, however, this is not conclusive and requires further study.
Can trigeminal neuralgia go away or be cured?
In some cases, trigeminal neuralgia can go into spontaneous remission for several years. However, this is usually a lifelong disease. In terms of having pain relieved from treatment, generally microvascular decompression can provide the longest relief, but there are more risks associated with this procedure. For example, it requires the skull to be opened up and carries the risks of major surgery and general anaesthesia use.
To find out more about trigeminal neuralgia, make an appointment with an expert.

