
What are my options if I don’t qualify for laser eye surgery? A guide to lens implantation
Written by:Implantable Collamer Lenses (ICLs) work a bit like contact lenses implanted into your eye. ICL implantation is an effective and safe way of correcting your vision, and a very good alternative if your spectacle prescription is out of range for safe laser vision correction. Over half a million ICLs have been implanted since 1992, and every year the number of patients choosing this option increases. Mr Bruce Allan, a leading ophthalmologist, explains what ICLs are and how they work.
LASIK, the dominant contemporary technique, is based on laser reshaping of the cornea. This works wonderfully well for many patients, but higher corrections require a greater depth of tissue removal, and there is a limit to the amount of corneal tissue that can be removed safely. So for many patients with higher refractive errors (typically -8.00D and above; +4.00D and above), alternative techniques based on lens implantation are more suitable. A number of different lens implants have been developed for correcting high refractive errors and the ICL is the safest of these.
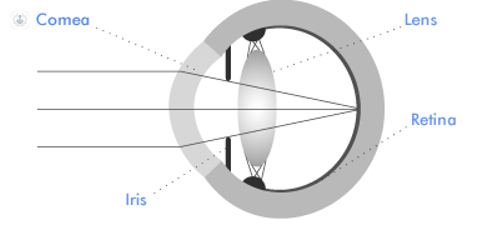
In high myopia (>-8.00D) the eye has too much focusing power. Without glasses, light from objects further than 1/8th of a metre away from the eye is focused in front of the retina, forming a blurred image. The ICL for high myopia (near-sightedness) (-8.00D and above) is a negative lens which acts to neutralise the excessive focusing power of the eye allowing clear vision in the distance.
The ICL for hypermetropia (far-sightedness) does the reverse. It is a positive lens that acts to neutralise insufficient focusing power. Astigmatism (uneven focusing power) is corrected using the toric ICL (TCL).
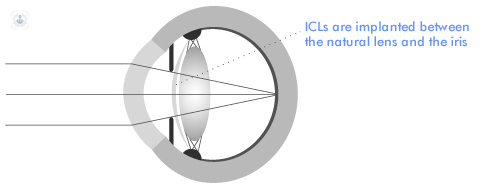
ICL surgery is based on tried and tested techniques for lens implantation developed in cataract surgery. A 3mm self-sealing valve type wound, which does not require sutures and does not diminish the strength of the eye wall, is used to enter the eye. The flexible ICL is then folded into an injecting device and injected through this wound. Specialised instruments are used to position the lens correctly, between the natural lens and the iris. The ICL effectively builds your contact lens or spectacle correction into the eye.
The ICL is made from a soft biocompatible gel material based on natural collagen. Because the lens is implanted within the eye, no cleaning is required. The operation can be performed under either local or general anaesthetic as a day case procedure (you do not need to stay in hospital overnight). You can normally see quite well within two days of the surgery. The eyes are operated on one week apart. After care is simple: drops four times a day for one month.
Outcomes following ICL implantation:
85% of patients with no other eye problems are able to see at the level of a normal non-spectacle wearer after ICL (or TCL) implantation at Moorfields Eye Hospital. Over 95% are able to see at the driving standard or better, and simple enhancement procedures are available for many patients who are not initially at this level.
The quality of vision for most patients is similar to that obtained in contact lenses. For patients with significant astigmatism, it is often better as TCLs provide better stability of vision than soft toric contact lenses. A realistic aim is to have vision that is good enough to participate in most sports and to socialise without glasses on. Many patients are spectacle free after surgery, but spectacles may still be required for some purposes – particularly for reading in patients over 40 years of age.
Am I too old for ICL implantation?
The American Food and Drug Administration (FDA) approves ICLs for patients 21-45 years of age. But what happens if you are over 45?
The short answer is nothing. Age related change in the eyes is gradual, and there are strong arguments for using ICLs, particularly for patients with high levels of short sight (myopia) well into the 50s. Most people start to notice the effects of ageing in the natural lens in their 40s. The lens gets less flexible, and reading vision deteriorates. But there is plenty of flexibility left, and newer ICLs with an extended depth of focus will soon be available to help you with the near range as you move on into your 50s.
Later in life, the lens gets less clear. A lens that is misty enough to cloud your vision is called a cataract. No-one gets a clearer lens as they age, and the main long-term risk of ICL implantation is developing cataracts sooner than you might do anyway. This is why refractive lens exchange (RLE), an operation identical to modern cataract surgery, is often offered if you are highly myopic and the wrong side of 45.
But latest generation ICLs encourage natural fluid circulation in the eye, and do not appear to accelerate cataract development. Also, important new research from France shows that the risk of retinal detachment after cataract surgery (or RLE) diminishes with age. ICL implantation presents no special problems for future cataract surgery, and does not increase your risk of retinal detachment. Even if it is just a stepping stone to cataract surgery later in life, ICL implantation is probably a safer option for your eyes than RLE for patients in mid-life with high myopia.
If you are interested in ICLs, make an appointment with a specialist.


