
ACL injuries: everything you need to know
Escrito por:Tears and sprains to the anterior cruciate ligament have been the bane of many an athlete’s career. While we have often heard of footballers and the like having these injuries in the newspaper, you may not know exactly what this ligament is or how you can deal with an injury to it. Top orthopaedic surgeon Mr Arjuna Imbuldeniya is here with a handy guide to this common sports injury.

What is the anterior cruciate ligament?
The anterior cruciate ligament (ACL) is one of the four main ligaments in the knee which work together to provide knee stability (the others are the posterior cruciate ligament [PCL], medial collateral ligament [MCL] and lateral collateral ligament [LCL]). The ACL is located in the middle of the knee and runs diagonally from the back of the femur (thigh bone) to the front of the tibia (shin bone). It prevents your tibia from moving excessively forward in relation to the femur and stops excessive inward rotation of the knee.
What causes anterior cruciate ligament injury?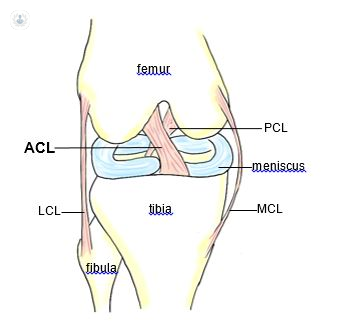
Injuries to the ACL include sprains and complete or partial tears, although complete tears are the most common.
ACL injuries usually occur as a result of twisting or pivoting injuries to the knee, such as stopping and changing direction quickly whilst running or jumping. Because of this, ACL injuries are common in sports such as football, basketball, tennis, volleyball and skiing, which involve turning and twisting movements. The ACL can also be torn following direct impact to the knee during contact sports such as rugby, but this is less common.
ACL injuries are generally more common in women than in men due to differences in knee joint anatomy, muscle bulk and because the female hormone oestrogen affects joint laxity.
What are the symptoms of anterior cruciate ligament injury?
Most people hear and/or feel a ‘popping’ in their knee when they injure their ACL. There is also usually immediate pain, especially on weight-bearing, and you may experience swelling within the first 6 hours, a reduced range of movement in the knee and feeling that the joint is unstable (‘giving way’ whilst walking or during physical activity).
Can you still walk if you have a torn anterior cruciate ligament?
Yes. Some people can live and function normally with a torn ACL, especially with good physiotherapy. Most people, however, find it causes their knee to feel painful or unstable and they may have difficulty walking, running or ascending/descending stairs on their injured leg.
How do you treat an anterior cruciate ligament injury?
Initial first aid treatment for a torn ACL includes resting the knee, applying ice and compression to it and taking anti-inflammatory and pain-relieving medications to help reduce pain and swelling. Using crutches whilst walking can also help to keep the weight off your knee.
You should see a consultant orthopaedic surgeon as soon as possible – ideally one who specialises in knee ligament injuries – to confirm the diagnosis and take you through all the appropriate treatment options. You are likely to require tests such as an MRI scan to help with this.
Not all torn ACLs require surgery; this will depend on whether you have symptoms of instability (the knee ‘giving way’) or if you like to participate in sports. Surgery is usually required if you hope to get back to physical activity, and can be performed four to six weeks after injury. This allows for the swelling and inflammation in the knee to settle, along with preventing joint stiffness.
Whether you are planning to have surgery or not, physiotherapy is important in ACL rehabilitation. Mobility and strengthening exercises help to improve muscle bulk around the knee in order to improve its stability, and to get your range of movement back to normal.
If you are going to have surgery on your torn ACL, it is important to have physiotherapy beforehand to optimise your knee muscles and movements in order to get the best results from your operation – this has been shown to improve overall outcomes.
The definitive management for a torn ACL with instability is reconstructive surgery, where your surgeon removes the damaged ACL and replaces it with tissue to help a new ligament grow in its place. This tissue usually comes from either one or two of your own hamstring tendons or part of your patellar or quadriceps tendon, although sometimes artificial or donor ligaments can be used instead. The tissue is held in place at either end using bony plugs, screws or other fixation devices such as suspensory buttons or bone staples.
Can the anterior cruciate ligament repair itself?
No. Unlike torn muscles, a torn ACL cannot heal by itself even though your knee may feel better after a couple of weeks of rest. Returning to physical activity without having it checked risks re-injury and damage to other structures in the knee, such as the meniscus, articular cartilage or other ligaments, which could also potentially accelerate wear and tear in the knee (osteoarthritis).
After surgery you will be able to walk without crutches by around 6 weeks, and with regular physiotherapy patients can often get back to sports again within 9 months to a year after their operation.

