
Improving tear production to treat dry eye syndrome
Escrito por:Dry eye is a multifactorial disease that is caused by poor tear production, an imbalance in the fats released from the eyelids that are used to stabilise the tear film and inflammation of the eye. Hence, treatment is not as simple as just adding extra tear drops if the other aspects have not been controlled adequately. Recent studies have confirmed that the other aspects may be sometimes more important than the tear production itself. Professor Sunil Shah, an award-winning ophthalmologist explains how tear production works and how dry eye syndrome can be managed.

There are two main types of dry eye – aqueous deficient (from low production of tears) and evaporative (from increased loss), however, these are just two ends of a spectrum and the vast majority of cases are a combination of aqueous deficient and evaporative forms. Hence, treatment has to be aimed at the various aspects of this multifactorial disease.
There are no easy ways to directly stimulate tear production at present, although devices are appearing which can stimulate tear production through stimulation of nerves within the nose. TrueTear® is one such device that is inserted up the nose and provides a gentle electrical stimulus which causes both immediate and more sustained tearing. Additionally, various operations to bring nerves to the lacrimal gland have been tried but are only reserved for special cases.
How do our eyes produce tears?
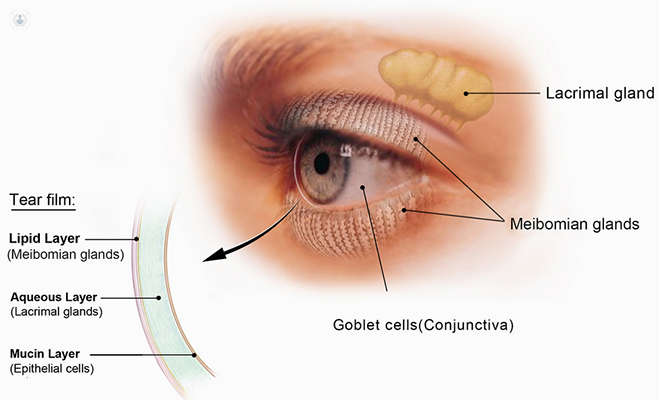
There is basal production and reflex production, both from the lacrimal gland which is situated above the outside part of the eye. The tears then run from the upper outer part of the eye to the lower middle part of the eye and then drain down the lacrimal punctum (a drainage hole). Then the tears run down the nasolacrimal duct into the back of the throat. This is why if you put in eye drops, you can sometimes taste the drops you put in the eye.
What can cause tear production to be insufficient?
One of the causes is because of a reduced sensation of the cornea - one of the most common causes being LASIK surgery which cuts corneal nerves and hence reduces sensation. This may also happen in other forms of eye surgery. Damage to the ducts which deliver the tears from the lacrimal gland from scarring diseases of the eye or chemical burns can also reduce tear production. A number of drugs such as antihistamines, b-blockers and some psychotropic drugs can cause a reduction in tear production. A common cause of reduced tear production is infiltration of the lacrimal gland by autoimmune diseases, such as in Sjogren’s syndrome.
How can tear production or tear evaporation be improved?
Dry eye treatment needs to address each of the underlying causes, so a good medical history needs to check for the possibility of general health problems and medication contributing to the dry eye. A common occurrence is acne rosacea.
Eye drops:
- Nerve stimulation is not freely available and hence the management of dry eye involves the addition of artificial tears that address the increased concentration of the tears (hyperosmolality). There are different types of drops depending on the severity of the problem and what is required, and there are even sprays. Some of the drops are much more watery and don’t last very long and some have fat in them to help stabilise the tear film.
Basic cleaning:
- Blepharitis is often present in addition to the dry eye and needs separate management – this may need basic cleaning. A device called BlephEx® can be used for cleaning the eyelashes or using treatments with tea tree oil based products like Cliradex®.
Meibomian gland dysfunction:
- This is a problem with the fat producing glands of the eyelid, which is often underdiagnosed and undertreated. This can benefit from treatment with heat bags to soften the fat in the glands, allowing them to be expressed. The glands can be squeezed to get the excess fat out of the glands and to open partially blocked glands. This can sometimes be helped with LipiView® to view the glands and LipiFlow® to express them.
Intense pulsed light (IPL):
- One of the biggest new treatments I have found is intense pulsed light. This was originally used to treat acne rosacea and then found to benefit dry eye. We now have instruments designed specifically for treatment of dry eye. This is a simple, non-invasive treatment on the eyelids that, after a course of three treatments, has been shown to reduce dry eye. I even use this prior to surgery now in patients with borderline or frank dry eye to almost eliminate dry eye problems after surgery.
Inflammation:
- The final treatment of the cause of dry eye is treatment of the inflammation associated with dry eye. All dry eye has inflammation that may need separate treatment. One can use steroid drops on a short-term basis to reduce the inflammation. If longer-term treatment is needed, then one needs to use either Restasis® or Ikervis® (cyclosporine) drops.
How can dry eyes be distinguished from an allergic eye reaction to something?
Your ophthalmologist can easily determine the difference between dry eyes and an allergic reaction as what they can see in the eye on examination is completely different (of course one can have both at the same time).
Why are women more prone to developing dry eye syndrome?
This is felt to be hormonal changes that cause dry eyes to be more common in women. The hormone changes have many effects, including effects on the fat producing glands and also on the production of tears.
If you suffer from irritated and dry eyes, make an appointment with an expert to see what your treatment options are.

